Anesthesia Records - Why Bother?
- NAVAS

- May 11, 2019
- 4 min read
Why is record keeping so important for the anesthetist?

There are many people out there who say that while working to anesthetize their patient they are so busy trying to wear so many “other hats” that record keeping is the least important of the many things they are trying to do. To this I say I UNDERSTAND. I have been there; we often wear so many hats while working that they begin to feel tight on our temples. But also remember as an extension of our veterinarian we need to ensure we are keeping their legal records properly.
Now I know many of you may be thinking, heavy sigh Lindsey this is going to slow me down. How on earth am I as the only Tech/Nurse in the whole prep and OR area - and sometimes what feels like the entire Earth - to be expected to anesthetize the patient, prep the OR, shave the pet, monitor said pet, AND RECORD THE VITALS while making sure the patient is alive????? This may seem like an exaggeration, but I have been in this exact situation more than once in my many years in my more than adequately staffed hospitals.
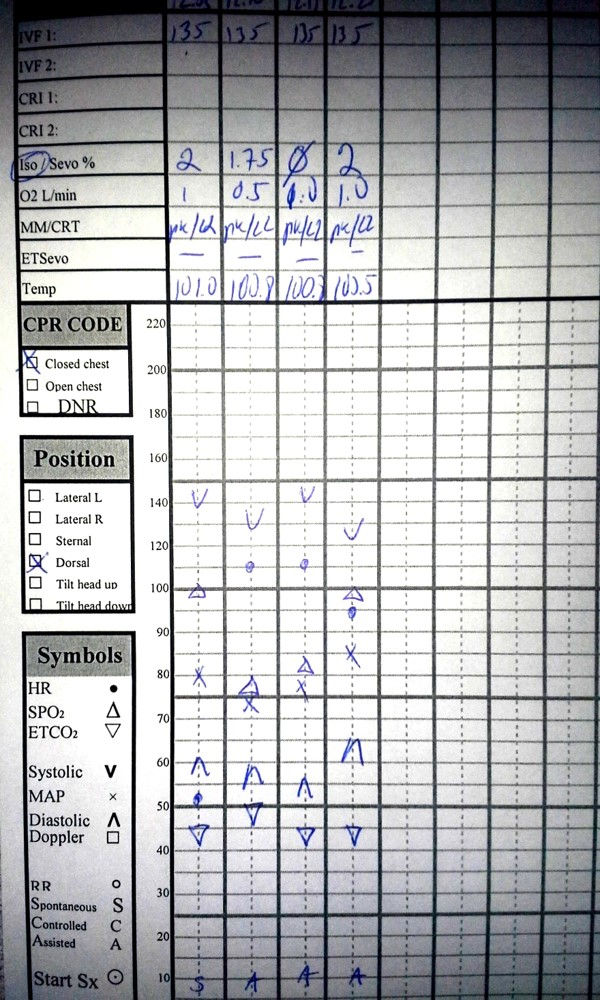
The above situation may seem hard but when you slow down the logistics and look closely at the point of keeping an anesthetic record, you will understand why it is vitally important (see what I did there 😊) to record patient parameters under anesthesia.
Anesthetic records are a part of every patient's medical record, which, from a legal standpoint means it is one of the most important documents we as technicians/nurses can create. Unfortunately, there may be some cases when your record keeping may be viewed as a representation of your DVMs overall ability to provide patient care.
Since some records keep a combination of electronic medical records (EMR ) and manually recorded anesthetic episodes, here is a refresher of what is means to actually write on a medical record.
Medical records should only be written in black or blue ink. Any mistakes should be crossed out with a single line and initialed by the person doing so. One should NEVER use white out to fix a mistake, as this may be viewed as an attempt to cover up a medical mistake if litigation ever occurs.
What should be included in anesthesia records? All premedications, induction agetns, antibiotic,s emergency medications and the patient’s responses should be cleared delineated. All medications administered should be recorde with full names (eg "torb" is slang and this medication should be written as "butorphanol" with dosages and adminsitration times written clearly. It is preferred to record the administered amount of both milligrams and milliliters given. The initial of the staff member and route of administration should also be noted as well.
All IV fluids or procedures performed during the anesthetic event (central line placement, arterial catheter), the size the endotracheal tube as well as the size and location of the blood pressure cuff should be noted as well. What size IV catheter was placed and where. All final anesthetic records should be signed by the staff who participated in the care of the patient.
Now for those of you still taking paper medical chart vitals it only takes 30 seconds to 2 minutes to record all your patients’ vitals. And for those using EMR devices attached to your monitor it takes no time. The ACVAA recommends that vitals be recorded a minimum of every 5-10 minutes during the anesthetic period (note however that the patient should be physically monitored continuously and without interruption). During critical cases it may be necessary to have more than one staff member available to keep proper records and care for the patient. Also remember many monitors also keep historical trends and have recall buttons you can use to record missed vitals as well.
While doing paperwork I try to think “Would this make sense to someone else?”. I like to use my forms to work toward perfection for my patients. When they come back next time, I pull my previous forms. How did things go last time? What drugs did I use and how did they work? What could I change to make the patient more comfortable? Were there any intraoperative issues with blood pressure? If so could I change something to help prevent this? How did my patient recover? What was the temperature like during the procedure? Should I spend more time pre-warming? What about recovery: calm, comfortable, and smooth? Or do we need to change the approach?
There I so much valuable information we can gather from anesthesia forms from the minute we administer premedications and place an IV catheter, induce and intubate to the minute you transfer the patient into the care of another staff member - it is amazing to think about. Sometimes we get so caught up in the routines of procedures and the day to day flow of things that I think we forget to record what seems normal to us. This “normal” can be so important when viewed in the eyes of another, especially if it is someone who is trying to find fault in your hospital's care.

In closing I look at it this way: if someone looks over a form two years from now, would they be able to read it and have a pretty good sense of what happened from the beginning to the end of the anesthetic event? If the answer is yes, I am pleased with my record keeping, if no, then I can - and should - improve!
Here are some sources for anesthesia records that you may be able to adapt to your clinical setting:
And the ACVAA.org has monitoring guidelines for small animal and equine patients here: http://www.acvaa.org/docs/Position_Statements



Lindsey Howard's mention of the 30 seconds to 2 minutes for vitals really stuck with me, alongside the rule about only using black or blue ink-it's those concrete details that make the logistics feel tangible Image to Image AI
The carrot-collecting objective in Poor Bunny adds a risk-versus-reward element. Going for more carrots increases your score but also puts you in greater danger.
Excellent! Will share with my students!